Post by Admin on Apr 8, 2020 5:12:48 GMT
Respiratory virus shedding in exhaled breath and efficacy of face masks
Nancy H. L. Leung, Daniel K. W. Chu, Eunice Y. C. Shiu, Kwok-Hung Chan, James J. McDevitt, Benien J. P. Hau, Hui-Ling Yen
Respiratory virus infections cause a broad and overlapping spectrum of symptoms collectively referred to as acute respiratory virus illnesses (ARIs) or more commonly the ‘common cold’. Although mostly mild, these ARIs can sometimes cause severe disease and death1. These viruses spread between humans through direct or indirect contact, respiratory droplets (including larger droplets that fall rapidly near the source as well as coarse aerosols with aerodynamic diameter >5 µm) and fine-particle aerosols (droplets and droplet nuclei with aerodynamic diameter ≤5 µm)2,3. Although hand hygiene and use of face masks, primarily targeting contact and respiratory droplet transmission, have been suggested as important mitigation strategies against influenza virus transmission4, little is known about the relative importance of these modes in the transmission of other common respiratory viruses2,3,5. Uncertainties similarly apply to the modes of transmission of COVID-19 (refs. 6,7).
Some health authorities recommend that masks be worn by ill individuals to prevent onward transmission (source control)4,8. Surgical face masks were originally introduced to protect patients from wound infection and contamination from surgeons (the wearer) during surgical procedures, and were later adopted to protect healthcare workers against acquiring infection from their patients. However, most of the existing evidence on the filtering efficacy of face masks and respirators comes from in vitro experiments with nonbiological particles9,10, which may not be generalizable to infectious respiratory virus droplets. There is little information on the efficacy of face masks in filtering respiratory viruses and reducing viral release from an individual with respiratory infections8, and most research has focused on influenza11,12.
Here we aimed to explore the importance of respiratory droplet and aerosol routes of transmission with a particular focus on coronaviruses, influenza viruses and rhinoviruses, by quantifying the amount of respiratory virus in exhaled breath of participants with medically attended ARIs and determining the potential efficacy of surgical face masks to prevent respiratory virus transmission.
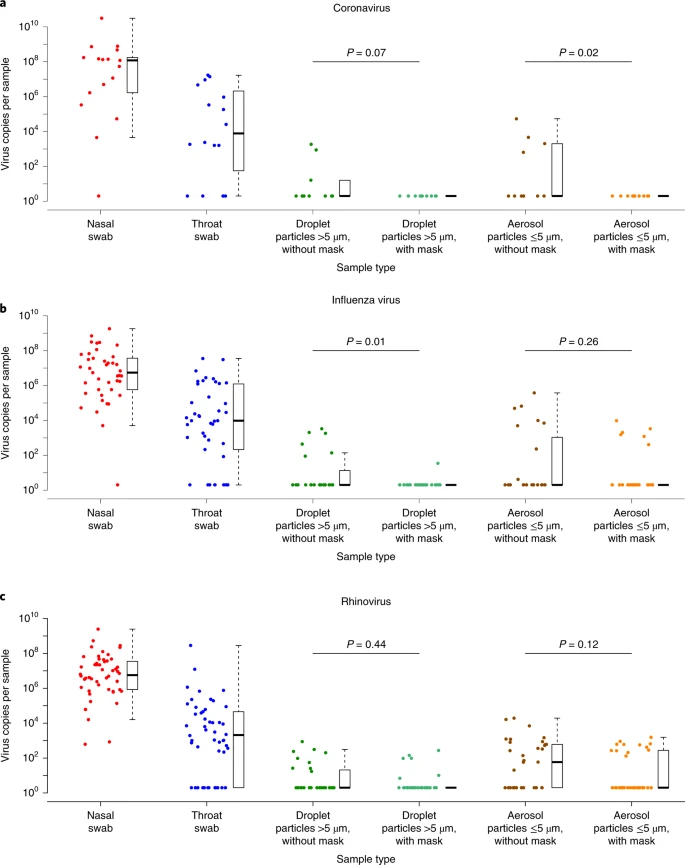
Fig. 1: Efficacy of surgical face masks in reducing respiratory virus shedding in respiratory droplets and aerosols of symptomatic individuals with coronavirus, influenza virus or rhinovirus infection.
Results
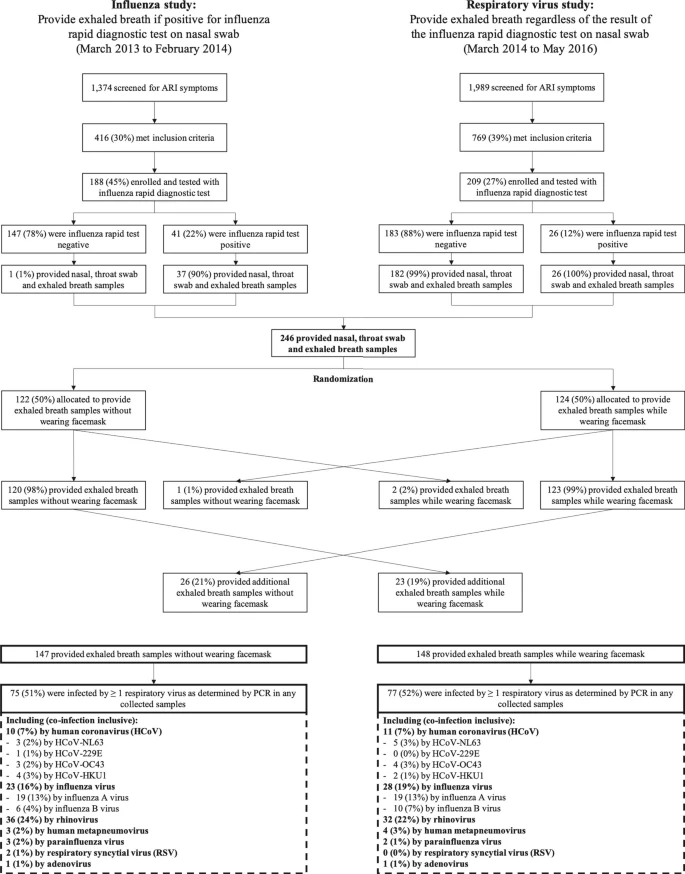
We screened 3,363 individuals in two study phases, ultimately enrolling 246 individuals who provided exhaled breath samples (Extended Data Fig. 1). Among these 246 participants, 122 (50%) participants were randomized to not wearing a face mask during the first exhaled breath collection and 124 (50%) participants were randomized to wearing a face mask. Overall, 49 (20%) voluntarily provided a second exhaled breath collection of the alternate type.
Infections by at least one respiratory virus were confirmed by reverse transcription PCR (RT–PCR) in 123 of 246 (50%) participants. Of these 123 participants, 111 (90%) were infected by human (seasonal) coronavirus (n = 17), influenza virus (n = 43) or rhinovirus (n = 54) (Extended Data Figs. 1 and 2), including one participant co-infected by both coronavirus and influenza virus and another two participants co-infected by both rhinovirus and influenza virus. These 111 participants were the focus of our analyses.
There were some minor differences in characteristics of the 111 participants with the different viruses (Table 1a). Overall, 24% of participants had a measured fever ≥37.8 °C, with patients with influenza more than twice as likely than patients infected with coronavirus and rhinovirus to have a measured fever. Coronavirus-infected participants coughed the most with an average of 17 (s.d. = 30) coughs during the 30-min exhaled breath collection. The profiles of the participants randomized to with-mask versus without-mask groups were similar (Supplementary Table 1).
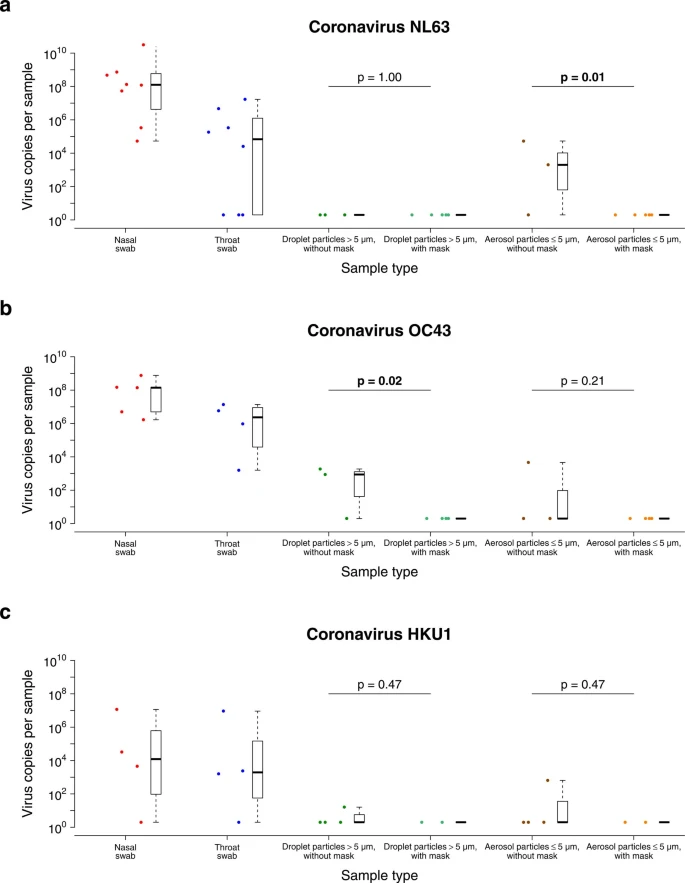
We tested viral shedding (in terms of viral copies per sample) in nasal swabs, throat swabs, respiratory droplet samples and aerosol samples and compared the latter two between samples collected with or without a face mask (Fig. 1). On average, viral shedding was higher in nasal swabs than in throat swabs for each of coronavirus (median 8.1 log10 virus copies per sample versus 3.9), influenza virus (6.7 versus 4.0) and rhinovirus (6.8 versus 3.3), respectively. Viral RNA was identified from respiratory droplets and aerosols for all three viruses, including 30%, 26% and 28% of respiratory droplets and 40%, 35% and 56% of aerosols collected while not wearing a face mask, from coronavirus, influenza virus and rhinovirus-infected participants, respectively (Table 1b). In particular for coronavirus, we identified OC43 and HKU1 from both respiratory droplets and aerosols, but only identified NL63 from aerosols and not from respiratory droplets (Supplementary Table 2 and Extended Data Fig. 3).
Nancy H. L. Leung, Daniel K. W. Chu, Eunice Y. C. Shiu, Kwok-Hung Chan, James J. McDevitt, Benien J. P. Hau, Hui-Ling Yen
Respiratory virus infections cause a broad and overlapping spectrum of symptoms collectively referred to as acute respiratory virus illnesses (ARIs) or more commonly the ‘common cold’. Although mostly mild, these ARIs can sometimes cause severe disease and death1. These viruses spread between humans through direct or indirect contact, respiratory droplets (including larger droplets that fall rapidly near the source as well as coarse aerosols with aerodynamic diameter >5 µm) and fine-particle aerosols (droplets and droplet nuclei with aerodynamic diameter ≤5 µm)2,3. Although hand hygiene and use of face masks, primarily targeting contact and respiratory droplet transmission, have been suggested as important mitigation strategies against influenza virus transmission4, little is known about the relative importance of these modes in the transmission of other common respiratory viruses2,3,5. Uncertainties similarly apply to the modes of transmission of COVID-19 (refs. 6,7).
Some health authorities recommend that masks be worn by ill individuals to prevent onward transmission (source control)4,8. Surgical face masks were originally introduced to protect patients from wound infection and contamination from surgeons (the wearer) during surgical procedures, and were later adopted to protect healthcare workers against acquiring infection from their patients. However, most of the existing evidence on the filtering efficacy of face masks and respirators comes from in vitro experiments with nonbiological particles9,10, which may not be generalizable to infectious respiratory virus droplets. There is little information on the efficacy of face masks in filtering respiratory viruses and reducing viral release from an individual with respiratory infections8, and most research has focused on influenza11,12.
Here we aimed to explore the importance of respiratory droplet and aerosol routes of transmission with a particular focus on coronaviruses, influenza viruses and rhinoviruses, by quantifying the amount of respiratory virus in exhaled breath of participants with medically attended ARIs and determining the potential efficacy of surgical face masks to prevent respiratory virus transmission.
Fig. 1: Efficacy of surgical face masks in reducing respiratory virus shedding in respiratory droplets and aerosols of symptomatic individuals with coronavirus, influenza virus or rhinovirus infection.
Results
We screened 3,363 individuals in two study phases, ultimately enrolling 246 individuals who provided exhaled breath samples (Extended Data Fig. 1). Among these 246 participants, 122 (50%) participants were randomized to not wearing a face mask during the first exhaled breath collection and 124 (50%) participants were randomized to wearing a face mask. Overall, 49 (20%) voluntarily provided a second exhaled breath collection of the alternate type.
Infections by at least one respiratory virus were confirmed by reverse transcription PCR (RT–PCR) in 123 of 246 (50%) participants. Of these 123 participants, 111 (90%) were infected by human (seasonal) coronavirus (n = 17), influenza virus (n = 43) or rhinovirus (n = 54) (Extended Data Figs. 1 and 2), including one participant co-infected by both coronavirus and influenza virus and another two participants co-infected by both rhinovirus and influenza virus. These 111 participants were the focus of our analyses.
There were some minor differences in characteristics of the 111 participants with the different viruses (Table 1a). Overall, 24% of participants had a measured fever ≥37.8 °C, with patients with influenza more than twice as likely than patients infected with coronavirus and rhinovirus to have a measured fever. Coronavirus-infected participants coughed the most with an average of 17 (s.d. = 30) coughs during the 30-min exhaled breath collection. The profiles of the participants randomized to with-mask versus without-mask groups were similar (Supplementary Table 1).
We tested viral shedding (in terms of viral copies per sample) in nasal swabs, throat swabs, respiratory droplet samples and aerosol samples and compared the latter two between samples collected with or without a face mask (Fig. 1). On average, viral shedding was higher in nasal swabs than in throat swabs for each of coronavirus (median 8.1 log10 virus copies per sample versus 3.9), influenza virus (6.7 versus 4.0) and rhinovirus (6.8 versus 3.3), respectively. Viral RNA was identified from respiratory droplets and aerosols for all three viruses, including 30%, 26% and 28% of respiratory droplets and 40%, 35% and 56% of aerosols collected while not wearing a face mask, from coronavirus, influenza virus and rhinovirus-infected participants, respectively (Table 1b). In particular for coronavirus, we identified OC43 and HKU1 from both respiratory droplets and aerosols, but only identified NL63 from aerosols and not from respiratory droplets (Supplementary Table 2 and Extended Data Fig. 3).