

Post by Admin on Feb 26, 2021 0:30:27 GMT
3.4. The RS Is Associated With Severity of COVID-19 in the Cohort of Spanish Patients
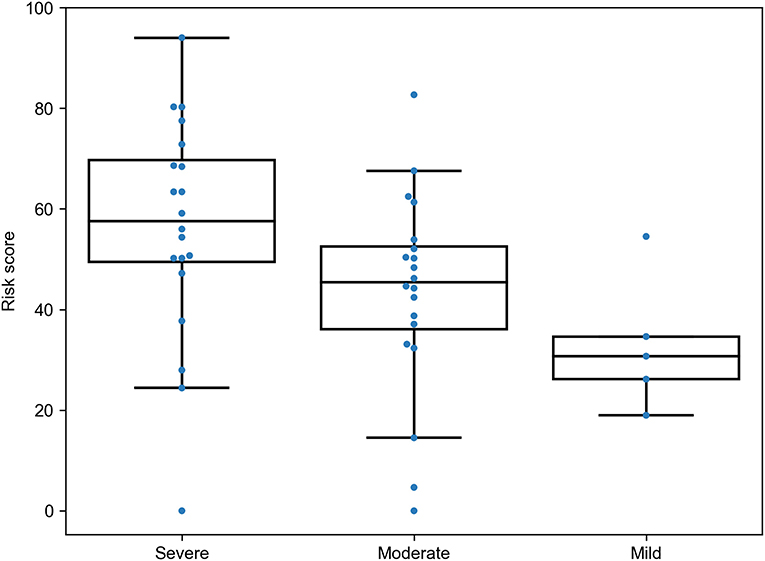
To see whether the proposed RS was associated with different patterns of the disease severity, we re-analyzed data from a recently published study on the role of HLA class I genotypes in COVID-19 in a cohort of Spanish patients (12). The data included genotypes of patients with severe (n = 20), moderate (n = 20), and mild (n = 5) SARS-CoV-2 infection. The RS model was applied to the data with no re-tuning of coefficients, and the same PCA weights were used for cohort-specific alleles. As a results, we found statistically significant dominance of RSs in patients with severe symptoms compared to moderate (U test p = 0.0157) and mild (p = 0.0161) patients, while, despite the matching direction, no statistical significance was found for the comparison of patients with moderate and mild infection (p = 0.0926), possibly due to the low sample size (Figure 5). Thus, the developed model allowed us to find dependencies between HLA class I genotypes and severity of the disease in the independent patient cohort from another population.
Figure 5. Risk score (RS) in groups of severe, moderate, and mild COVID-19 patients from the Spanish cohort
3.5. Human Leukocyte Antigen Class I Homozygosity Is a Double-Edged Sword for COVID-19 Risk
When analyzing the high RS group, we noticed that more than half (five out of eight) deceased patients containing HLA-A*01:01 alleles were homozygous by this allele, while the medium group had not a single individual homozygous by HLA-A*01:01 (Fisher's exact test p = 0.0103). The distribution of homozygous individual by HLA-A*01:01 among the groups of deceased patients and the control group proved its negative role. It turned out that the distribution in the deceased group (4 out of 26 patients who died <60, and 1 out of 85 patients who died >60) leads to two statistically significant differences: p-value of Fisher's exact test comparing the adults group with the elderly group equals 3.10 × 10−3, and p-value of the test comparing the adults group and the control group equals 0.0104 (8 out of 428 members of the control group were homozygous by HLA-A*01:01). However, the difference between the elderly group and the control group is statistically insignificant (p = 0.155). Interestingly, there were no other statistically significant differences in the distribution of homozygosity between the groups.
Generally, the average age of death for patients homozygous by any allele was significantly less compared to heterozygous ones (Mann-Whitney U test p = 6.45 × 10−3, Supplementary Figure 2). Also, the fraction of homozygous patients was higher in the group of deceased adults (42.3%) compared both to elderly patients (15.3%, Fisher's exact test p = 6.03 × 10−3) and the control group (19.2%, p = 9.80 × 10−3). Difference between the elderly and control groups was not statistically significant (p = 0.448).
However, the low risk group also contained homozygous individuals: all homozygosity cases by HLA-A*02:01 (six cases) and HLA-A*03:01 (two cases) alleles were associated with low risk. These assignments were in agreement with age of death: only one patient homozygous by HLA-A*02:01 had not passed the 60 years age of death threshold. Thus, homozygosity by HLA class I genes is generally associated with poor prognosis except for some alleles like HLA-A*02:01 and HLA-A*03:01 with “relevant” peptide-binding profiles.
To see whether the proposed RS was associated with different patterns of the disease severity, we re-analyzed data from a recently published study on the role of HLA class I genotypes in COVID-19 in a cohort of Spanish patients (12). The data included genotypes of patients with severe (n = 20), moderate (n = 20), and mild (n = 5) SARS-CoV-2 infection. The RS model was applied to the data with no re-tuning of coefficients, and the same PCA weights were used for cohort-specific alleles. As a results, we found statistically significant dominance of RSs in patients with severe symptoms compared to moderate (U test p = 0.0157) and mild (p = 0.0161) patients, while, despite the matching direction, no statistical significance was found for the comparison of patients with moderate and mild infection (p = 0.0926), possibly due to the low sample size (Figure 5). Thus, the developed model allowed us to find dependencies between HLA class I genotypes and severity of the disease in the independent patient cohort from another population.
Figure 5. Risk score (RS) in groups of severe, moderate, and mild COVID-19 patients from the Spanish cohort
3.5. Human Leukocyte Antigen Class I Homozygosity Is a Double-Edged Sword for COVID-19 Risk
When analyzing the high RS group, we noticed that more than half (five out of eight) deceased patients containing HLA-A*01:01 alleles were homozygous by this allele, while the medium group had not a single individual homozygous by HLA-A*01:01 (Fisher's exact test p = 0.0103). The distribution of homozygous individual by HLA-A*01:01 among the groups of deceased patients and the control group proved its negative role. It turned out that the distribution in the deceased group (4 out of 26 patients who died <60, and 1 out of 85 patients who died >60) leads to two statistically significant differences: p-value of Fisher's exact test comparing the adults group with the elderly group equals 3.10 × 10−3, and p-value of the test comparing the adults group and the control group equals 0.0104 (8 out of 428 members of the control group were homozygous by HLA-A*01:01). However, the difference between the elderly group and the control group is statistically insignificant (p = 0.155). Interestingly, there were no other statistically significant differences in the distribution of homozygosity between the groups.
Generally, the average age of death for patients homozygous by any allele was significantly less compared to heterozygous ones (Mann-Whitney U test p = 6.45 × 10−3, Supplementary Figure 2). Also, the fraction of homozygous patients was higher in the group of deceased adults (42.3%) compared both to elderly patients (15.3%, Fisher's exact test p = 6.03 × 10−3) and the control group (19.2%, p = 9.80 × 10−3). Difference between the elderly and control groups was not statistically significant (p = 0.448).
However, the low risk group also contained homozygous individuals: all homozygosity cases by HLA-A*02:01 (six cases) and HLA-A*03:01 (two cases) alleles were associated with low risk. These assignments were in agreement with age of death: only one patient homozygous by HLA-A*02:01 had not passed the 60 years age of death threshold. Thus, homozygosity by HLA class I genes is generally associated with poor prognosis except for some alleles like HLA-A*02:01 and HLA-A*03:01 with “relevant” peptide-binding profiles.