Post by Admin on Aug 23, 2023 1:55:49 GMT
Postacute sequelae of COVID-19 at 2 years
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection can lead to postacute sequelae in multiple organ systems, but evidence is mostly limited to the first year postinfection. We built a cohort of 138,818 individuals with SARS-CoV-2 infection and 5,985,227 noninfected control group from the US Department of Veterans Affairs and followed them for 2 years to estimate the risks of death and 80 prespecified postacute sequelae of COVID-19 (PASC) according to care setting during the acute phase of infection. The increased risk of death was not significant beyond 6 months after infection among nonhospitalized but remained significantly elevated through the 2 years in hospitalized individuals. Within the 80 prespecified sequelae, 69% and 35% of them became not significant at 2 years after infection among nonhospitalized and hospitalized individuals, respectively. Cumulatively at 2 years, PASC contributed 80.4 (95% confidence interval (CI): 71.6–89.6) and 642.8 (95% CI: 596.9–689.3) disability-adjusted life years (DALYs) per 1,000 persons among nonhospitalized and hospitalized individuals; 25.3% (18.9–31.0%) and 21.3% (18.2–24.5%) of the cumulative 2-year DALYs in nonhospitalized and hospitalized were from the second year. In sum, while risks of many sequelae declined 2 years after infection, the substantial cumulative burden of health loss due to PASC calls for attention to the care needs of people with long-term health effects due to SARS-CoV-2 infection.
Main
More than 3 years after the onset of the COVID-19 global pandemic, a wave of evidence suggests that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection can lead to postacute sequelae in pulmonary and broad array of extrapulmonary organ systems1,2,3,4,5,6,7,8,9,10,11,12—including increased risks and burdens of cardiovascular disorders, neurologic and mental health disorders, metabolic disorders (diabetes and dyslipidemia), kidney disorders and gastrointestinal disorders. The risks and burdens of these sequelae have been assessed in the few months to a year after the onset of infection1,2,3,4,5,6,7,8,9,10,11,12. Few studies with longer follow-ups (longer than 1 year) examined a limited set of symptoms in individuals with COVID-19 or focused exclusively on neurologic sequelae13,14,15,16,17. Except for work discussed in ref. 13 that mapped risk trajectories of neurologic and psychiatric sequelae and showed substantial heterogeneity in their risk profiles, it remains unclear whether and over what time horizon the risk of postacute sequelae of SARS-CoV-2 attenuates and becomes not significant. A comprehensive assessment of the risks and burdens of postacute sequelae of COVID-19 (PASC) across care settings of the acute infection in the 2 years after the infection is not yet available. Addressing this knowledge gap would deepen our understanding of the postacute and long-term health trajectories of people who had SARS-CoV-2 infection and will inform post-COVID care strategies.
In this study, we use the US Department of Veterans Affairs (VA) national healthcare databases to build a cohort of 138,818 US veterans who survived the first 30 days of SARS-CoV-2 infection and a control group of 5,985,227 users of the US Veterans Health Administration (VHA) with no evidence of SARS-CoV-2 infection. These cohorts were followed longitudinally for 2 years to estimate the risks of death, hospitalization and prespecified array of 80 pulmonary and extrapulmonary sequelae of SARS-CoV-2 throughout the 2-year follow-up and cumulatively at 2 years in mutually exclusive groups according to care setting during the acute phase of the disease (nonhospitalized and hospitalized) and in the overall cohort.
Results
There were 138,818 and 5,985,227 participants in the COVID-19 and noninfected control groups, respectively. The COVID-19 group had a mean age of 60.91 years (s.d.: 15.96), and 11.41% of participants were female. The control group had a mean age of 62.82 years (s.d.: 16.84), and 9.93% of participants were female. Median follow-up time was 715 days (interquartile range (IQR): 687–720) in the COVID-19 group and 719 days (IQR: 690–720) in the control group, with a total of 255,119 and 11,181,224 person-years of follow-up, respectively, which altogether corresponded to 11,436,344 person-years of follow-up. Demographic and health characteristics of the COVID-19 and noninfected control groups before and after inverse probability weighting for baseline covariates are presented in Supplementary Tables 1 and 2.
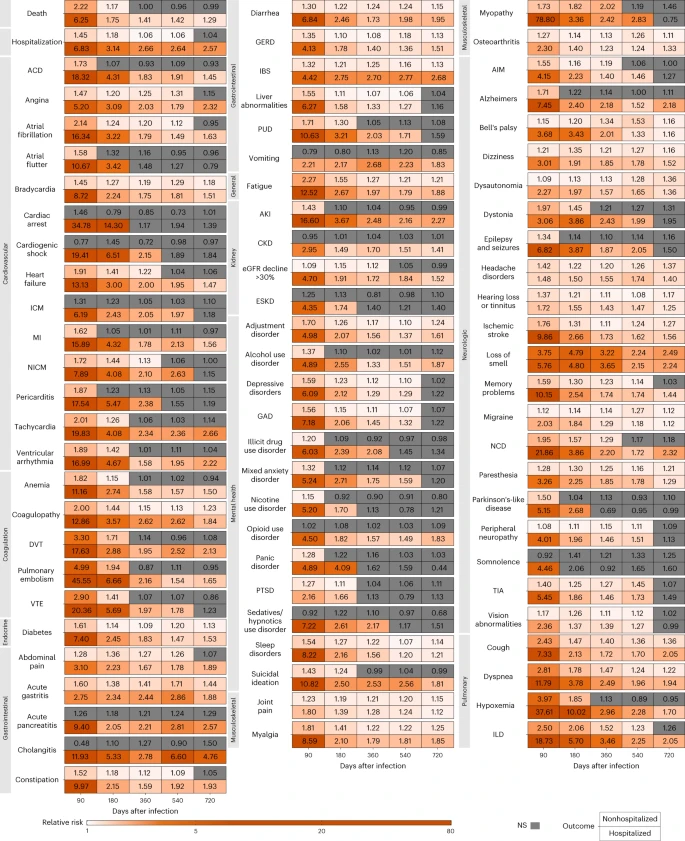
We examined risks of death, hospitalization and a set of 80 prespecified postacute COVID-19 sequelae, as well as sequelae aggregated by organ system and aggregated as an overall outcome of PASC by care setting (nonhospitalized (n = 118,238) and hospitalized (n = 20,580) during the acute phase of SARS-CoV-2 infection) and overall (n = 138,818) during the following five time periods of the postacute phase of the disease: 30–90, 91–180, 181–360, 361–540 and 541–720 days after a SARS-CoV-2 infection.